
Dr. Hisham Burezq, BSc MD FRCSC FAAP
Consultant Plastic & Reconstructive Surgeon
Consultant Pediatric Plastic Surgeon
Canadian Board and fellowship in plastic surgery
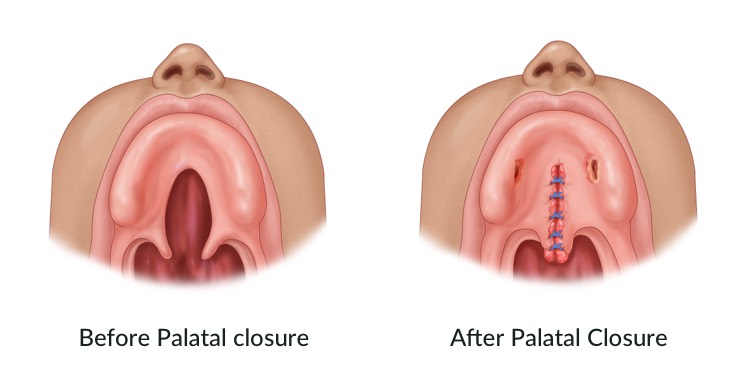
The roof of the mouth (palate)forms during 6-9 weeks of pregnancy. A cleft palate forms when tissues don’t connect in the midline. An opening or split occurs in the palate as a result. A cleft palate can include the soft palate(the back mobile part of the palate)only or also include the hard palate(the bony anterior part of the palate). A cleft palate can occur in isolation or include a cleft lip as well in one side or both sides of the mouth. It is considered one of the most common birth defects. It may occur as an isolated case or it can be associated with many conditions such as the cleft lip or inherited genetic syndromes.
Having a child with clefts can be very upsetting for parents, but thankfully it can be corrected at a high success rate. In most children, a series of surgeries can restore the normal function of the palate.
How will cleft lip and palate affect your child:
Children with cleft lip with or without cleft palate face a variety of challenges, depending on the type and severity of the cleft.
- Difficulty in feeding. Feeding is one of the most immediate problems after birth. While most babies with a cleft lip can be breastfed, the cleft palate may make breastfeeding difficult. Babies with cleft palate will need feeding through a specialized bottle.
- Ear infections and hearing loss. Children with cleft palate are particularly at risk of developing middle ear fluid and hearing loss, especially if the procedure is delayed after the age of one year old.
- Dental problems. If the cleft extends across the upper gums, tooth growth may be affected.
- Speech difficulties. Since the palate is used to form sounds, the development of normal speech may be affected and speech may appear very nasally (Nasality).
- The challenges of coping with the medical condition. Children with clefts may experience social, emotional and behavioral problems due to the differences in appearance and the intensive medical attention pressure.
Before going to the Hospital:
- Visiting the Anesthesiologist a week before the procedure is important to make sure that the child is ready for surgery.
- The child usually hospitalized for 2 days, and in some cases needs to spend his first night in the ICU; due to the procedure’s site and its relation to breathing.
- The child should refrain from eating for 8 hours before the procedure.
Procedure:
- It takes approximately 2.5 hours to 3 hours under general anesthesia.
- The child will be given painkillers after surgery while in hospital.
-
After the Procedure
- It is important for the child to sleep on his stomach or on one side for the first two days; in order to get rid of any secretions or blood after the surgery.
- Lifting the child’s head after the procedure using a pillow starting from the second day and for 24-48 hours is useful for relieving the swelling resulting from the procedure.
- small amounts of blood comes out of the mouth and nose in the first two days following the procedure, which is expected and not a cause for concern.
- The child may start snoring for a long time.
- How the child should eat after the procedure:
- We start with water and glucose (sugar) in the first two times gently using a syringe.
- Afterwards, the child will drink light liquids (interspersed with light) for two days, such as apple and grape juices and milk.
- The child will then be allowed to drink any type of liquids.
- Starting from the fourth day after the procedure, the child will eat soft food and stays away from eating anything solid for a month after the procedure.
- Your child will be discharged home when they are able to drink plenty of fluids and are comfortable and pain free at day1-2 after surgery
After your child is discharged from the hospital, return to the emergency room if they show the following:
- Stops eating and drinking.
- Suffers from a fever.
- Suffers from a severe bleeding from the mouth.
- Clear unpleasant smell from the mouth.
Possible Complications from the Procedure:
The procedure’s success rate is high and reaches 80-90%, but like other procedures, this one may result in rare complications, including:
- The need to enter the ICU to monitor their breathing, and if this occurs, it will be due to swelling in the pharynx and tongue after the procedure, and usually for one day.
- Delayed wound healing. It may be due to the presence of bacteria inside the mouth, which may result in a cleft palate that requires another surgery to be performed 6-12 months after the first procedure.
- The occurrence of bleeding during or after surgery, with an incidence rate not exceeding 0.5%, but for the sake of caution, blood will be prepared for the child before the procedure.
- The need for another procedure at the age of 5-8 years old to treat the nasality in 30% of the children, if they do not respond to the therapy conducted by the Speech and Hearing Specialist.
- General complications related to general anesthesia, which are very rare.
Helpful Links
Downloads





